Content
- Transgender-inclusive healthcare in Tamil Nadu
- Holding up GLASS to India; securing stewardship to tackle AMR
- Centre releases draft Seeds Bill; farm outfits cautious, industry welcomes it
- SC bats for protection of pristine sal forest in Jharkhand’s Saranda
- Workplace stress linked to rising cases of diabetes among adults
- Why Hepatitis A deserves a place in India’s Universal Immunisation Programme
Transgender-inclusive healthcare in Tamil Nadu
Why is this in News?
- Article highlights Tamil Nadu’s pioneering model in transgender-inclusive public healthcare.
- Showcases India’s first State-level integration of gender-affirming care into universal health coverage.
- WHO is preparing a global case study (2025) documenting Tamil Nadu’s model.
- Updates on progress: 8 Gender Guidance Clinics (GGCs), 5,200+ enrolments, and 600+ surgeries/hormone procedures under CMCHIS-PMJAY.
Relevance
- GS 2 – Welfare of Vulnerable Sections
Rights of transgender persons; health equity; inclusive public services - GS 2 – Health & Social Justice
Universal Health Coverage; insurance inclusion; role of State governments - GS 2 – Governance & Policy Implementation
State-level innovations; administrative reforms; public service delivery - GS 1 – Society
Gender identity, stigma, discrimination, social inclusion
Basics
- “Leave no one behind” = Core commitment under UN SDGs and Universal Health Coverage (UHC).
- Transgender persons are recognised as a marginalised group needing targeted interventions under:
- Transgender Persons (Protection of Rights) Act, 2019
- NHM (Tamil Nadu)
- State Policy for Transgender Persons (2025)
Why do Transgender Persons Face Healthcare Barriers?
- Skill Gaps in Medical Workforce
- Majority clinicians untrained in transgender health.
- Overfocus on STI treatment & surgeries; neglect of preventive, reproductive, geriatric, mental health.
- Structural Exclusion
- Low access to education, formal employment, housing, social security → unstable income & no insurance.
- Discrimination in Healthcare Settings
- Stigma, ridicule, denial of services.
- Fear erodes trust → delayed care, medical complications.
- Documentation Barriers
- Identity mismatch, lack of supportive families, exclusion from ration cards/ID-based welfare.
- Intersectionality Effects
- Health deprivation overlaps with caste, poverty, homelessness.
What Has Tamil Nadu Done?
- 2008: Rajiv Gandhi Government General Hospital begins gender-affirming surgeries.
- 2008: India’s first Transgender Welfare Board created.
- 2018: NHM establishes Gender Guidance Clinics (GGCs) providing multidisciplinary care.
- 2025: 8 districts now host GGCs with free procedures.
- 2019–2024: 7,644 transgender individuals accessed GGC services.
Services Offered
- Hormone therapy
- Gender-affirming surgery
- Mental health counselling
- STI/HIV services
- Legal/identity support, social linkage
How Has Tamil Nadu Expanded Insurance Coverage?
- 2022: CMCHIS-PMJAY includes gender-affirming surgeries & hormone therapy.
- India = first South Asian country to integrate transgender care under UHC.
- Insurance Partner: United India Insurance Co. (5-year policy 2022–27).
- Advancing PMJAY TG Plus (which offers 50+ procedures):
- TN is 4 years ahead in implementation.
Key Reforms for Accessibility
- Removed income limit of ₹72,000.
- Waived need for ration card with transgender person’s name.
- Addressed exclusion from families, lack of proof, stigma.
Outcomes (as of Oct 2025)
- 5,200+ enrolled under CMCHIS-PMJAY.
- 600+ underwent surgeries/hormone therapy.
- Care provided in 12 empanelled hospitals (public + private).
Policy & Legal Reforms Strengthening the Model
- 2019 Transgender Act (Sec 15): Mandates comprehensive healthcare.
- 2024: NHM trains GGC doctors on WPATH Standards of Care v8.
- Madras High Court Judgments:
- Recognised transgender marriages.
- Mandated curriculum reforms.
- Banned conversion therapy.
- Banned non-consensual intersex surgeries.
- Ordered reopening of GGCs post-COVID.
- Curbed police harassment.
- State Policy Framework
- 2019 TN Mental Health Care Policy
- 2025 State Policy for Transgender Persons: property rights, education, healthcare access.
What Challenges Remain?
- Limited Coverage & Geographical Reach
- Need statewide GGC expansion and district-level continuum of care.
- Lack of Comprehensive Health Manual
- Standard protocols for hormones, surgeries, follow-up, mental health missing.
- Monitoring & Regulation Gaps
- Empanelled hospitals need strong oversight to prevent malpractice/exploitation.
- Mental Health Coverage
- Needs integration into insurance packages; high prevalence of depression, anxiety, violence trauma.
- Provider Competency
- Requires periodic training, certification, accountability mechanisms.
- Grievance Redressal Mechanisms
- Currently weak; community often fears reporting discrimination.
- Limited Research & Data
- Need for State-level epidemiological data on transgender health.
- Persistent Social Prejudice
- Requires cross-sectoral interventions: education, policing, media, families.
- Community Participation
- Policy design, implementation, monitoring must involve transgender-led organisations.
Conclusion
- Tamil Nadu has created India’s most advanced model of transgender-inclusive healthcare with early adoption of gender-affirming services, strong insurance coverage, progressive jurisprudence, and community engagement.
- However, lasting equity requires continuous investment, wider coverage, accountability, and institutionalising transgender persons as partners—not beneficiaries—in the health system.
Holding up GLASS to India; securing stewardship to tackle AMR
Why is this in news?
- WHO released its Global Antimicrobial Resistance Surveillance System (GLASS) 2025 report in mid-October 2025.
- India identified as one of the worst AMR hotspots globally.
- Highlights a severe rise in antibiotic-resistant infections, especially in ICUs.
- Kerala’s progress and India’s slow national AMR implementation reignited policy debates.
- Published just ahead of World AMR Awareness Week (18–24 November).
Relevance
- GS 3 – Science & Technology / Biotechnology
Antimicrobial resistance, global surveillance systems (GLASS) - GS 3 – Health & Disease Burden
AMR as a major public health threat; ICU infections; One Health approach - GS 3 – Environment
Pharma effluent regulation, environmental determinants of AMR
Basics
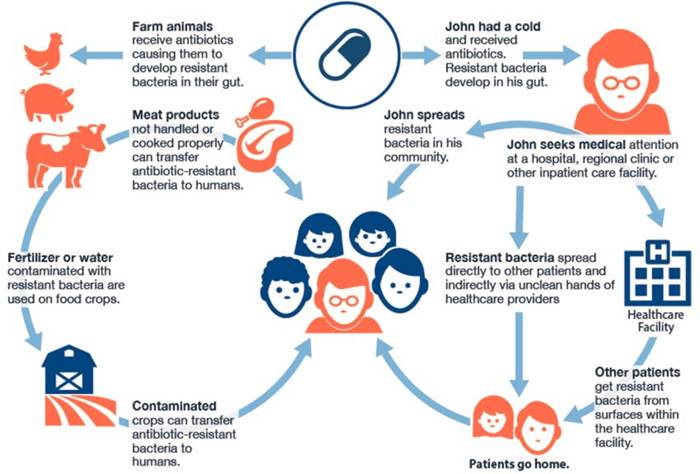
- Antimicrobial resistance (AMR) occurs when microbes evolve to resist antibiotics → infections become harder or impossible to treat.
- AMR is driven by human, animal, agriculture, and environmental pathways → a One Health problem.
- GLASS is WHO’s global AMR monitoring system, operational in 100+ countries; India joined in 2017.
Key global findings (GLASS 2025)
- 1 in 6 infections globally resistant to commonly used antibiotics.
- South-East Asia shows the steepest rise; India is disproportionately affected.
- High resistance among critical pathogens: E. coli, Klebsiella pneumoniae, Staphylococcus aureus.
- WHO flags a modest but insufficient improvement in the global antibiotic development pipeline.
India-specific findings
- 1 in 3 infections in India in 2023 were antibiotic-resistant.
- Highest resistance burden in ICUs for E. coli, Klebsiella, and MRSA.
- Strong AMR drivers in India:
- Over-the-counter antibiotics
- Self-medication and incomplete courses
- Contaminated pharma effluents and hospital waste
- Weak enforcement of antibiotic regulations
- GLASS notes progress but flags underfunding, uneven surveillance, and weak coordination.
Current efforts in India
- National Programme on AMR Containment.
- ICMR’s AMRSN / i-AMRSS network.
- NCDC’s NARS-Net.
- 2019 ban on colistin in animal feed (significant but long-term impact).
Major weaknesses identified
- Surveillance bias:
- Overdependence on tertiary hospitals → overestimation of AMR; weak data from rural/primary-care settings.
- Underfunding:
- No long-term investment in AMR research, stewardship, or diagnostics.
- Poor One Health coordination.
- NAP-AMR implementation slow:
- 2017 plan remains mostly unexecuted in many States.
- Public awareness extremely low → AMR remains an abstract concept for most Indians.
Expert assessments
Abdul Ghafur
- India’s AMR levels are among the highest globally.
- True national estimates require integrating 500+ NABL labs + primary/secondary hospital microbiology.
V. Ramasubramanian
- Surveillance centres must be geographically spread; without regional representation, conclusions are distorted.
Ella Balasa
- Public needs relatable narratives; humanising AMR is essential for behavioural change.
Antibiotic development pipeline (critical analysis)
Global pipeline trends
- WHO 2024 pipeline report:
- 97 candidates in clinical & preclinical stages (up from 80 in 2021).
- Only 12 of 32 traditional antibiotics are innovative (new class or new mechanism).
- Just 4 candidates target WHO priority MDR Gram-negative pathogens.
India’s status
- CDSCO has approved four new antibiotic candidates in the last two years.
- Six more have global approval.
Limitations
- Pipeline is still too small to address global AMR.
- Limited innovation; low access in LMICs.
- Most new drugs do not target carbapenem-resistant Gram-negatives.
Features needed in next-generation antibiotics
- New mechanisms bypassing current resistance.
- Dual formulations (IV + oral).
- Activity against highest-priority MDR pathogens.
- Safe, affordable, and aligned with stewardship guidelines.
- Low likelihood of inducing further resistance.
Global and industry-side initiatives
AMR Industry Alliance
- Promotes development of new antibiotics and diagnostics.
- Supports responsible antibiotic manufacturing.
- Works on equitable access, especially in LMICs.
Funding gaps
- Surveillance and innovation receive intermittent and inadequate funding.
- Need sustained national investment in AMR research, stewardship, and public awareness.
Kerala model
- Only State with a fully operational AMR State Action Plan.
- Kerala AMR Strategic Action Plan (2018) adopts a strong One Health model.
- AMRITH (2024) stops over-the-counter antibiotic sales.
- State antibiogram shows a slight reduction in AMR levels.
- Goal: antibiotic-literate Kerala by December 2025.
Other significant interventions
- 2019 colistin ban in poultry/livestock → expected long-term benefits.
- Need uniform enforcement across all States.
What India must do (priority recommendations)
Surveillance
- Build a representative national network using NABL labs.
- Strengthen microbiology capacity in district and primary-care hospitals.
Stewardship
- Nationwide ban on OTC antibiotic sales.
- Standardised antibiotic guidelines across hospitals.
- Functional stewardship committees in all tertiary and secondary facilities.
Environment
- Regulate pharma effluents and medical waste.
- Mandatory antimicrobial pollutant monitoring.
Awareness
- Large-scale community orientation on AMR.
- Humanised public campaigns (schools, digital media).
Innovation
- Incentives for new antibiotic classes.
- Academia-industry collaborations.
- Public funding for early-stage R&D.
Governance
- Accelerate implementation of NAP-AMR (2017).
- Strong State-level monitoring and coordination.
Conclusion
- India’s AMR crisis is severe, escalating, and under-monitored.GLASS 2025 reinforces that resistance is rising faster than countermeasures, and progress remains fragmented.
Kerala demonstrates that structured One Health interventions, regulatory enforcement, and public literacy can reduce resistance trends. - India now needs integrated surveillance, strict stewardship, environmental control, innovation incentives, and long-term funding to prevent a future where routine infections again become untreatable.
Centre releases draft Seeds Bill; farm outfits cautious, industry welcomes it
Why in news?
- The Union government has released a new draft Seeds Bill, 2025, after two failed attempts to pass similar legislation in 2004 (UPA) and 2019 (NDA) due to farmer opposition.
- It aims to replace the Seeds Act, 1966 and the Seeds (Control) Order, 1983.
- Government claims alignment with current agricultural and regulatory needs, including seed quality control and liberalised imports.
- Public comments open till December 11.
Relevance
- GS 3 – Agriculture
Seed regulation, quality control, farmer access, seed imports - GS 3 – Economy
Private sector role in seed industry; liberalisation; ease of doing business - GS 2 – Governance / Policy
Legislative reforms; regulatory modernisation; stakeholder conflicts
What are “seeds laws” in India?
- Seeds laws regulate:
- Quality parameters (germination %; genetic purity; physical purity; seed health).
- Certification processes (Indian Minimum Seed Certification Standards).
- Registration of seed dealers and varieties.
- Liability for seed failure.
- The Seeds Act, 1966 is considered outdated:
- Focused on public-sector dominance.
- Lacks frameworks for modern hybrids, GM events, private R&D, and global seed trade.
Key provisions of the draft Seeds Bill, 2025
- Mandatory registration:
- Every seed dealer must register with the State government before selling or exporting/importing seeds.
- Quality regulation:
- Seeds sold must meet minimum certification standards for germination, purity, traits, health.
- Regulation of sale to ensure declared performance.
- Liberalisation:
- Greater freedom for seed imports, enabling access to global varieties.
- Decriminalisation:
- Minor offences decriminalised to reduce compliance burden.
- Serious violations retain strong penalties.
- Farmer protection:
- Ensures farmers’ access to high-quality seeds at affordable rates.
- Aims to prevent losses due to substandard seeds.
Why earlier attempts (2004 and 2019) failed
- Farmer groups opposed:
- Mandatory registration and certification seen as restricting farmer-saved seeds.
- Fear of greater corporate control over the seed market.
- Concerns around liability provisions favouring companies.
- Bills were withdrawn after widespread protests, especially in Punjab, Haryana, Maharashtra, Telangana.
Farmers’ perspective
- Seen as industry-friendly:
- “Bill favours seed companies and facilitates ease of doing seeds business” (BKU-Ekta Ugrahan).
- Key concerns:
- Could lead to higher seed prices.
- Risk of monopolisation by MNCs/private breeders.
- Stronger regulation might apply more to farmers than companies.
- Fear of indirect control over farmer-saved and exchanged seeds via registration norms.
Seed industry perspective
- Welcomed as a modernising move, especially by the Federation of Seed Industry of India.
- Benefits to industry:
- Clearer regulatory regime.
- Decriminalisation reduces business risk.
- Liberalised imports expand breeding and hybridisation possibilities.
- Predictability for private investment.
Larger policy context: why regulate seeds more tightly now?
- India’s seed market size: ₹25,000–27,000 crore; private sector share: 65–70%.
- Issues:
- Quality failures cause 10–30% yield loss depending on crop.
- Spurious seeds cases frequently reported in cotton, paddy, vegetables.
- Need to integrate global seed variety testing, DUS criteria, and digital traceability.
Critical analysis
Strengths
- Modernises a 60-year-old law.
- Better consumer protection through quality benchmarks.
- Enables innovation and global germplasm flow.
- Rationalises penal provisions → encourages private R&D.
Concerns
- May unintentionally promote corporate dominance in seeds.
- Registration rules could affect:
- farm-saved varieties,
- community seed systems.
- Liberalised imports risk entry of high-cost foreign varieties → price inflation.
- No clarity on seed liability and compensation mechanisms — historically the most contentious aspect.
- Risk of conflict with:
- PPV&FRA, 2001 (farmers’ rights),
- Biodiversity Act, 2002 (access to genetic resources).
Governance risks
- States’ capacity to run robust registration and testing systems remains weak.
- Enforcement uneven across India → inconsistent protection for farmers.
SC bats for protection of pristine sal forest in Jharkhand’s Saranda
Why in news?
- The Supreme Court has directed the Jharkhand government to declare 31,468.25 hectares (314 sq. km.) of the Saranda forest as a wildlife sanctuary.
- This ends the State’s reluctance and its earlier proposal to declare only 24,941.64 hectares due to concerns over mining and infrastructure.
- The court emphasised the State’s constitutional duty to protect ecologically significant areas and balance conservation with sustainable mining.
Relevance
- GS 3 – Environment & Biodiversity
Sal forest ecosystem; wildlife sanctuary declaration; threatened species - GS 3 – Conservation vs Development
Mining–ecology conflict; sustainable mining; iron ore reserves - GS 2 – Judiciary / Constitutional Provisions
Public trust doctrine; State’s duty to protect forests

Basics: where and what is Saranda?
- Location: West Singhbhum district, Jharkhand.
- Known as one of the world’s most pristine sal forests.
- Ecological features:
- Dominant sal (Shorea robusta) ecosystem.
- Home to endemic sal forest tortoise, four-horned antelope, Asian palm civet, wild elephants.
- Social context:
- Inhabited for centuries by Ho, Munda, Uraon and allied Adivasi communities.
- Livelihoods deeply tied to minor forest produce and cultural traditions.
Why is the area contentious?
- Saranda forest division also contains 26% of India’s iron ore reserves.
- SAIL and Tata Steel depend critically on mining in this region.
- Judicial declaration of the entire 314 sq. km. as a sanctuary could:
- Restrict or reshape mining operations.
- Affect employment in mining-linked areas.
- Require reevaluation of several leases.
Key observations of the Supreme Court
- State’s duty:
- Forests and wildlife must receive statutory protection where ecologically significant.
- The State cannot “run away from its duty to declare” such areas.
- Balanced approach:
- Conservation must coexist with sustainable iron ore mining, not eliminate it.
- Sanctuary notification does not automatically extinguish tribal rights.
- Community protection:
- Court directed mass communication that individual and community forest rights under FRA, 2006 will not be adversely affected.
- Ecological significance:
- Court stressed the unique sal ecosystem, biodiversity richness, and presence of threatened species.
Government’s position (as per hearings)
- Initially proposed declaring only 24,941.64 hectares due to:
- “Vital public infrastructure” in the remaining area.
- Concerns about halting mining.
- Later clarified:
- The 31,468.25 hectares being considered had no mining, no non-forest use, and no prior diversion.
- After the court’s push, the government agreed to proceed with full notification.
Ecological significance
- Saranda is a high-integrity sal landscape—rare globally.
- Functions as a critical elephant habitat and corridor.
- Sanctuary status ensures:
- Stricter protection under the Wildlife (Protection) Act, 1972.
- Better control over fragmentation from roads, mining, and encroachments.
Mining–conservation tension
- Region’s mineral value is extremely high (26% national iron ore).
- Conservation imperatives clash with:
- Employment generation.
- Steel sector supply chains.
- Local economic activity.
- Court’s directive pushes for “sustainable mining + strict ecological zoning” rather than blanket bans.
Tribal rights and welfare
- FRA, 2006: Sanctuary notification cannot extinguish existing rights.
- Court acknowledged:
- Tribes are ecosystem stakeholders.
- Sanctuary declaration must not lead to displacement.
- Important shift from earlier models of exclusionary conservation.
Governance implications
- Sets a precedent:
- States must declare ecologically important areas even if economically sensitive.
- Strengthens judicial oversight over forest governance.
- Enhances application of:
- Precautionary principle
- Public trust doctrine
- Requires integrated landscape planning for:
- Mining zones
- No-go biodiversity zones
- Community rights areas
Workplace stress linked to rising cases of diabetes among adults
Why in news?
- New clinical observations and emerging Indian research show a sharp rise in workplace-stress–linked Type 2 diabetes, especially among young urban working adults.
- Doctors report increasing cases among tech, finance, customer service, healthcare and night-shift workers.
- The report is released in the context of World Diabetes Day, highlighting stress as a major but under-recognised metabolic risk factor.
Relevance
- GS 3 – Health / NCDs
Stress-induced Type 2 diabetes; metabolic disorders; India’s disease burden - GS 3 – Economy / Labour
Workplace wellness, productivity loss, occupational health risks - GS 1 – Society
Changing work culture; lifestyle transitions; urbanisation impacts
Basics: what is stress-linked diabetes?
- Prolonged workplace stress → chronic activation of cortisol and adrenaline.
- These hormones:
- Raise blood glucose
- Reduce insulin sensitivity
- Increase central (abdominal) fat
- Disrupt circadian rhythm (especially in shift workers)
- Result: Insulin resistance → pre-diabetes → Type 2 diabetes.
What the data shows ?
- India: 10.1 crore diabetics (ICMR–INDIAB, 2023).
- Tamil Nadu study: higher perceived stress = poorer glycaemic control + longer disease duration.
- Hospitals in Chennai & Bengaluru report earlier onset (30s–40s) even without excess dietary intake.
Clinical observations
Early metabolic signs (often ignored as “busy life”)
- Abdominal weight gain
- Daytime fatigue
- Fragmented sleep
- Increased cravings
- Borderline BP
- Mildly elevated triglycerides
- Rising post-meal sugars
Why they worsen unnoticed
- Normalisation of long work hours
- Sleep deprivation
- Irregular meals
- Sedentary desk culture
- High device dependence and constant “on-call” pressures
Why certain professions are high-risk
IT, Finance, Customer Support
- Long screen hours
- High cognitive load
- Deadline cycles
- Constant notifications
- Guilt about switching off devices
Healthcare
- Emotional labour + erratic schedules
Night-shift workers
- Circadian rhythm disruption
- Irregular meals → reduced insulin sensitivity
- Higher glucose variability despite good diet adherence
Pathophysiology: how stress translates to diabetes
- Chronic stress → persistent HPA axis activation.
- Elevated cortisol:
- Increases hepatic glucose output
- Promotes visceral fat accumulation
- Reduces muscle glucose uptake
- Adrenaline surges:
- Fluctuating post-meal sugars
- Sleep disruption
- End result: progressive insulin resistance.
Doctors’ insights from multiple hospitals
- More young adults (29–45 years) showing central obesity + borderline sugars.
- Women show higher incidence of stress-linked metabolic changes in recent studies.
- Many patients discover diabetes incidentally through routine tests.
- Stress management improves glycaemic stability even in medicated patients.
Workplace factors driving the trend
- No scheduled lunch breaks
- Prolonged sitting
- Excessive meeting loads
- Late-night logging
- Shift rotation gaps
- Poor sleep hygiene
- High job insecurity
- Multitasking pressure
Evidence-backed low-cost interventions
For workplaces
- Protected lunch breaks
- 5–10 minute movement gaps between meetings
- Restrictions on after-hours work communication
- Healthier cafeteria menus
- Predictable shift rotations
For individuals
- 7–8 hours sleep
- Mindfulness/therapy
- Structured daily routines
- Consistent meal timings
- Device-free downtime
- Walking meetings / micro-activity
Doctors emphasise: “Stabilising cortisol stabilises blood sugar.”
Overview
Public health significance
- Stress-linked diabetes is emerging as a non-traditional risk factor.
- Shifts diabetes from being purely lifestyle-driven to occupational-environment–driven.
- Raises concerns for India’s young workforce and productivity.
Economic implications
- Higher absenteeism and presenteeism
- Rising corporate healthcare costs
- Long-term burden on insurance systems
- Earlier onset → longer disease duration → higher complications
Gender dimension
- Women face dual stress exposures: workplace + unpaid care work.
- Increasing evidence of higher pre-diabetes progression rates in women under occupational stress.
Policy relevance
- Need for integration of occupational health within NCD programmes.
- Shift work regulation and circadian-friendly policies.
- Mandatory workplace wellness norms for high-risk sectors.
Behavioural challenge
- Stress is intangible → symptoms normalised.
- Requires awareness + employer accountability + clinical screening.
Why Hepatitis A deserves a place in India’s universal immunisation programme
Why in news?
- India is debating including the Typhoid Conjugate Vaccine (TCV) in the Universal Immunisation Programme (UIP).
- Experts argue that Hepatitis A vaccination deserves even higher priority because the disease burden is shifting toward adolescents and adults — groups at significantly higher risk of severe disease, including acute liver failure.
- The article highlights that an effective indigenous Hepatitis A vaccine exists, yet policy inclusion is pending.
Relevance
- GS 2 – Health / Immunisation
UIP expansion; vaccine policy; epidemiological transition - GS 3 – Public Health
Outbreak management; sanitation transition; acute liver failure - GS 2 – Governance & Policy
Evidence-based policymaking; cost-effectiveness; indigenous vaccine development
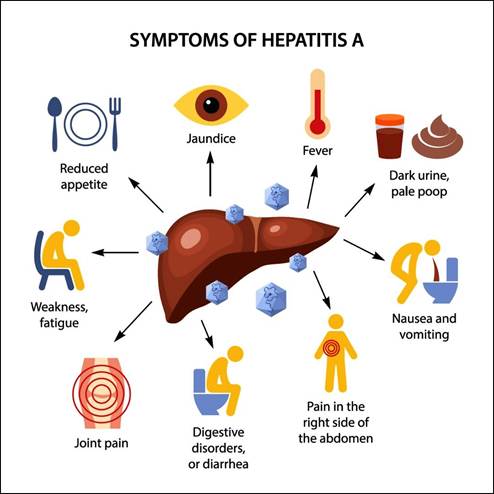
Basics: what is Hepatitis A?
- Acute viral liver infection typically mild in young children.
- Historically: >90% Indians exposed in childhood → lifelong immunity.
- Current shift: improved sanitation → fewer children infected early → more susceptible adolescents & adults.
- Severe disease in older age groups → acute liver failure, hospitalisation, deaths.
- No specific antiviral treatment → only supportive care.
Changing epidemiology
- Seroprevalence (protective antibodies) dropping from ~90% to <60% in many urban regions.
- Outbreaks reported in Kerala, Maharashtra, Uttar Pradesh, Delhi.
- Clusters of acute liver failure in hospitals show rising severity.
- Hepatitis A now an emerging public-health threat, not a benign childhood disease.
Hepatitis A vs Typhoid: key contrasts
Disease burden
- Typhoid mortality declining with antibiotics + sanitation.
- Hepatitis A rising in older children/adults → more severe outcomes.
Treatment
- Typhoid: antibiotics available; AMR emerging but treatable.
- Hepatitis A: no specific treatment, recovery depends entirely on supportive care.
Vaccine characteristics
- Hepatitis A vaccines:
- 90–95% efficacy
- Single dose for live vaccine
- Long-lasting (15–20 years to lifelong)
- No issues of waning immunity or resistance
- Typhoid vaccines: require multi-dose cycles in some settings; immunity relatively shorter.
Programmatic simplicity
- Hepatitis A vaccine is single-dose, easy to integrate with existing booster schedules.
- Indigenous product (Biovac-A by Biological E) has two decades of excellent use in private sector.
Cost-effectiveness
- Hepatitis A: high-cost outbreaks, expensive hospitalisation, severe disease in adults → strong economic rationale for universal vaccination.
- Typhoid: important but lower immediate cost-effectiveness because mortality has declined.
Why Hepatitis A deserves priority
- Growing susceptible population: fewer children infected early → rising young adult vulnerability.
- Severe disease profile: adult infection = higher hospitalisation + acute liver failure risk.
- No treatment: prevention via vaccination is the only effective shield.
- Low-hanging fruit:
- Single dose
- Long-term immunity
- Indigenous supply available
- Clear scientific evidence: declining antibodies + frequent outbreaks.
Recommended strategy for India
- Adopt a phased introduction, aligned with UIP’s proven approach:
- Start with States facing repeated outbreaks or low seroprevalence.
- Co-administer with DPT or MR boosters to use existing systems.
- Conduct periodic serosurveys to monitor immunity levels.
- Gradually expand to national scale.
Public health rationale
- Fits UIP tradition of proactive shifts (Hepatitis B, Rotavirus, Pneumococcal).
- Helps prevent avoidable severe disease and hospital burden.
- Reduces long-term healthcare costs by preventing liver complications early.
Overview
Epidemiological relevance
- The shift from early childhood exposure to adolescent vulnerability reflects India’s sanitation transition.
- Parallel seen previously in East Asia and Latin America before they introduced universal Hepatitis A vaccination.
- Without vaccination, India risks repeated outbreaks and rising adult mortality from acute liver failure.
Programmatic feasibility
- Single-dose administration makes planning efficient.
- Indigenous production ensures supply security and affordability.
- Can be rapidly scaled using existing UIP logistics.
Economic considerations
- Adult hospitalisations for Hep A are expensive (ICU care, liver monitoring, long recovery).
- Vaccination cost per child is low compared to treatment cost.
- Higher workforce productivity because adults are protected.
Policy gap
- Scientific consensus is strong, but policy action is lagging, unlike for TCV where debate is ongoing.
- No technical barrier: the missing piece is only political and administrative decision-making.